



Prostatectomy is a surgical procedure which partially or completely removes the prostate gland. It can be performed in different ways, depending on the initial diagnosis and advised treatment strategy. Frequently this procedure is performed to treat prostate cancer and in such case it is referred to as radical prostatectomy. It may be performed alone or combined with other types of treatment such as radiation, chemotherapy and hormone therapy.
Prostatectomy to treat prostate cancer requires the removal of the entire prostate, seminal vesicles, and surrounding lymph nodes.
There are different ways to approach the surgical procedure such as open radical prostatectomy, laparoscopic radical prostatectomy, and robot-assisted radical prostatectomy.
Table of Contents
Indications of Prostatectomy
The radical prostatectomy is recommended in patients with localized prostate cancer.
Simple prostatectomy is indicated for men with urinary symptoms and enlarged prostate glands. It can be performed with a different range of techniques. The surgery relieves the complications resulting from blocked urine flow such as urinary incontinence, a frequent need to urinate, difficulty starting urination, prolonged urination, nocturia, stopping and starting again while urinating, urinary retention. Usually, this procedure has a higher risk of complications and typically results in longer recovery time.
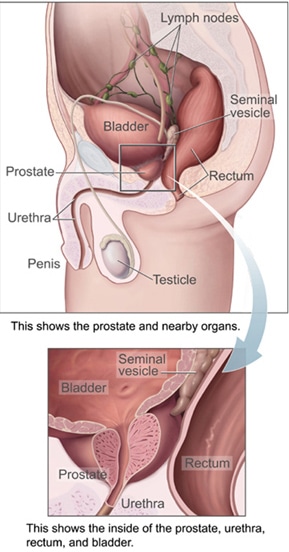
Created by US government agency National Cancer Institute [Public domain], via Wikimedia Commons
Prostatectomy procedure and techniques
A radical prostatectomy can be performed using different techniques, including:
- Robot-assisted radical prostatectomy. The urologist performs several small incisions in the lower abdomen with the aim to remove the prostate. The surgeon sits in the console, using the instruments attached to a robot. The robotic device allows a more accurate response to movement of the surgeon’s hands.
- Open radical prostatectomy. The urologist performs an incision in the lower abdomen to remove the prostate known as retropubic surgery
- Laparoscopic radical prostatectomy. The urologist performs several incisions in the lower abdomen and inserts special tools to remove the prostate.
- Transurethral resection of the prostate (TURP). Performed without external incisions and using a flexible tube (endoscope) inserted into the penis (urethra) to remove the prostate gland.
Before the surgery, the urologist will perform a comprehensive physical examination and will prescribe and perform a cystoscopy to evaluate the size of the prostate. Other laboratory tests sometimes are required with the aim to assess the kidney and liver function, the clotting profile and measure the prostate and the urine flow.
During the interview, the patient should explain if he or she is currently taking blood-thinning medications and nonprescription pain relievers, such as aspirin, any history of allergies. Usually, before the surgery, the doctor will recommend an enema, to clear the bowels.
Incisions for open and robotic prostatectomy
The incision for open prostatectomy is longer than the small incisions for robotic surgery
- Open prostatectomy: In these cases, one large incision is done in the abdomen
- Robotic prostatectomy: Surgeon will do between five to six small incisions to insert the surgical instruments in the belly. During this procedure, the urologist sits at a remote control console not far from the patient. The console shows a 3-D view of the abdomen. As a result, the surgeon will be able to visualize the procedure with greater details than the laparoscopic surgery. The robotic system allows more accurate incisions with a positive impact on the recovery time. The robotic approach usually enables nerve-sparing techniques with consequent preservation of the sexual potency and continence. Besides that, the patient often can return to daily activity, with minor restrictions in 15 days to one month after surgery. Robotic-assisted laparoscopic prostatectomy was first performed in 2000. It was popularized as a minimally invasive technique. In particular, this technique offered a 3-dimensional stereoscopic visualization, automatic finger-controlled movements with a range of motion surpassing that of the human hand. Clearly, this new technology has become the dominant method of surgical treatment for prostate cancer
- Open retropubic radical prostatectomy. The urologist performs an incision in the lower abdomen. After that, the surgeon makes a dissection of the prostate gland protecting the nerves and blood vessels with the aim to remove the prostate. The incision is finally sutured after the removal of the prostate. If we compare this type of surgery with other types of operation, we need to emphasize that retropubic prostate surgery has a lower risk of nerve damage already related to erectile dysfunction problems.
- Simple prostatectomy. The urologist can start the procedure with a cystoscopy. The surgeon will then insert a Foley catheter into the penis up to the bladder. The tube will evacuate the urine during the operation. The incision will be made below the navel. Once the surgeon has removed the part of the prostate responsible for the urinary symptoms, two temporary draining tubes will be inserted through the skin: one tube will be inserted directly into the bladder, and the other tube will drain the pelvic area.

BruceBlaus [CC BY-SA 4.0 (https://creativecommons.org/licenses/by-sa/4.0)], from Wikimedia Commons
Complications
The prostatectomy is a surgical procedure. The possible complications are active bleeding, urinary infection, urinary incontinence, Lymphocele, Erectile dysfunction, rectum injury and narrowing of the urethra.
A simple prostatectomy has a higher rate of complications and the recovery time is longer than other surgical procedures such as TURP known as transurethral resection of the prostate, laser PVP surgery or holmium laser prostate surgery known as HoLEP.
Some of the most common complications of TURP are the bleeding on the operation site, injury to adjacent structures, urinary incontinence, sexual impotence, dry orgasm, narrowing of the urethra or narrowing of the bladder neck.
Postoperative management
After surgery, the patient will receive intravenous analgesia. After the intravenous line is removed, the surgeon usually prescribes oral analgesics and anti-inflammatories.
The patient will go home after the surgery. The sutures will be removed after 15 days. Often the urinary catheter needs to be kept for five to ten days after surgery.
The physical activity level should be increased gradually. The patient can start with the usual routine after four to six weeks. During this time of recovery, it is not allowed to drive
The patient will be able to resume the sexual activity after recovering from surgery. Following a simple prostatectomy, the patient will experience an orgasm during the sexual intercourse, but little or no semen might come out (dry orgasm).
The Robot-assisted prostatectomy is the best available option in most cases. Several studies have shown that this intervention reduces pain and blood loss, diminish tissue trauma, reduce the hospital stay, and it has a positive impact on the recovery period. The patient usually returns to the regular activity, with only mild restrictions, 15 days or 1 month after the operation.
Open simple prostatectomy usually produces relief of the urinary symptoms. It is the most invasive method to treat an enlarged prostate, but the complications are not common.
References
- Herbert Lepor, MD, A Review of Surgical Techniques for Radical Prostatectomy. Rev Urol. 2005; 7(Suppl 2): S11–S17.
- Menon, Shrivastava A, Tewari A. Laparoscopic radical prostatectomy: conventional and robotic. 2005 Nov;66(5 Suppl):101-4.
- Fabio Castiglione, David J. Ralph,and Asif Muneer. Surgical Techniques for Managing Post-prostatectomy Erectile Dysfunction. Curr Urol Rep. 2017; 18(11): 90. Published online 2017 Sep 30. doi: 1007/s11934-017-0735-2
- Mikhail AA, Stockton BR, Orvieto MA, Chien GW, Gong EM, Zorn KC, Brendler CB, Zagaja GP, Shalhav AL. Robotic-assisted laparoscopic prostatectomy in overweight and obese patients. 2006 Apr;67(4):774-9. Epub 2006 Mar 29.
- Garg T, Young AJ, Kost KA, Park AM1, Danella JF1, Kirchner HL. Patient-reported quality of life recovery curves after robotic prostatectomy are similar across body mass index categories. Investig Clin Urol. 2017 Sep;58(5):331-338. doi: 10.4111/icu.2017.58.5.331. Epub 2017 Aug 3.
{kind=link}